What are Grand Mal Seizures?
Imagine first aid responders, dressed in red, running across the field in urgency on a typical day at summer camp. These are the series of events that I witnessed during my first week as a counsellor, hanging out with my cabin on that same field. Seeing all the commotion, I asked another counsellor, “what is going on?”
They responded, “a camper is having a seizure”.
Immediately, my mind went to the stereotypical images of what a seizure looks like: Jerking movements, eyes moving from side to side and muscles twitching.
I went home that night, opened my computer and fell into a rabbit hole of research on “what is a seizure?”
The first statistic that popped up on my screen was “about 1 in 10 people will have a seizure in their lifetime”. I was shocked to read this statistic and thought to myself, “IT’S THAT COMMON!?”
I later learned that there are many types of seizures. Some may present as blank stares into space, while others may present as the stereotypical seizures often seen on TV and that I thought of when I heard about the camper.
Grand mal seizures, also known as tonic-clonic seizures, are the most recognizable type of seizure. They account for 25% of all generalized seizures and often occur with epilepsy.
In this blog, I am going to write about how to recognize a tonic-clonic seizure, its causes, what happens in the brain and what you can do to help.
How to Recognize a Tonic-Clonic Seizure
Tonic-clonic seizures are a type of generalized seizure that results in a loss of consciousness and muscle contractions.
Tonic-clonic seizures may begin with a simple partial seizure, where the person may experience changes in sensation and mood. The partial seizure may then spread from one side of the brain to the other, resulting in a tonic-clonic seizure.
During the tonic phase:
Muscles stiffen and become rigid
The person may let out a cry or groan as the muscles in the body contract, forcing air out of the vocal cords.
Loss of consciousness
During the clonic phase:
The arms and legs begin to jerk rhythmically
Breathing may be limited
Blue lips or a dusky-looking face
The jerking movements will slow before the seizure stops and consciousness will gradually return.
After tonic-clonic seizures, the individual may experience the following symptoms:
Confusion
Drowsiness
Irritability
Loss of memory about the seizure episode
Headache
Todd paralysis (weakness on one side of the body, lasting a few minutes to a few hours)
How to Respond When You See Someone Having a Tonic-Clonic Seizure?
When I heard a camper was having a seizure, I was in shock. I thought to myself, what would I do if that was one of my own campers and truthfully, I did not know how to answer that question. I now understand how important it is to know how to respond when you encounter someone having a tonic-clonic seizure, as it could potentially save their life.
Do not touch or try to restrain the person when they are having a seizure.
Do not put anything in the individual’s mouth.
Do move objects away from the individual to minimize the risk of them injuring themselves.
Do time the seizures. Generally, tonic-clonic seizures last 1 to 3 minutes; however, if they last more than 5 minutes, or three seizures occur in a row, immediately call 911 for emergency help.
Do provide support to the individual once the seizure stops as they may feel confused or tired.
Causes
Tonic-clonic seizures can be caused by many conditions, such as:
Traumatic brain injury: Some people develop a seizure after a traumatic head injury
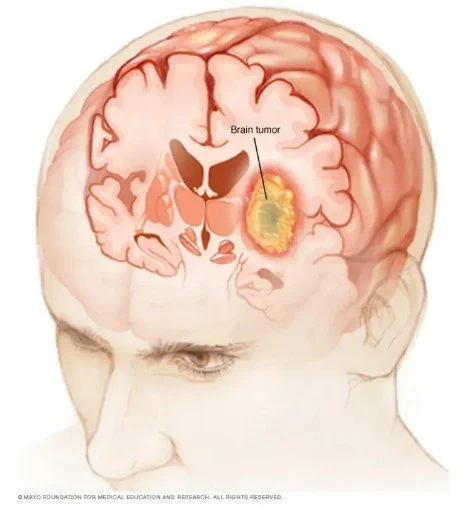
Brain conditions: Strokes and brain tumors may result in brain damage, causing seizures
Congenital or developmental factors: Genetic syndromes or blood vessels that do not fully develop within the brain can lead to a seizure
Metabolic problems: Low levels of blood glucose, sodium, calcium or magnesium may increase the likeness of having a seizure
Extreme lack of sleep
For a more extensive list on the causes of seizures, visit this link: https://www.epilepsy.com/causes
What Happens in the Brain?
Neurons within the brain communicate by transmitting electrical impulses from one neuron to another. In a healthy brain, neurons fire independently and at different times. Seizures occur when there is an abnormal release of electrical activity by a large group of neurons firing at the same time. In tonic-clonic seizures, both hemispheres of the brain are affected. The abnormal release of electrical activity interrupts normal brain function. The subcortical, cortical and brain stem networks are affected.
For more information on what happens in the brain during a seizure, watch this video: What Happens in Your Brain During a Seizure | WebMD
Diagnosis of Epilepsy
An electroencephalogram (EEG) is used to detect abnormalities in brain waves or electrical activity of the brain. EEG’s can be used to detect seizure activity in the brain as it will appear as spike-and-wave discharges on the EEG. The spike-and-wave discharges on the EEG result from synchronized bursts of neuronal firing that occur during a seizure. However, the sensitivity for an EEG to identify a seizure is less than 50% and therefore, a normal EEG does not rule out the possibility that the patient did not have a seizure.
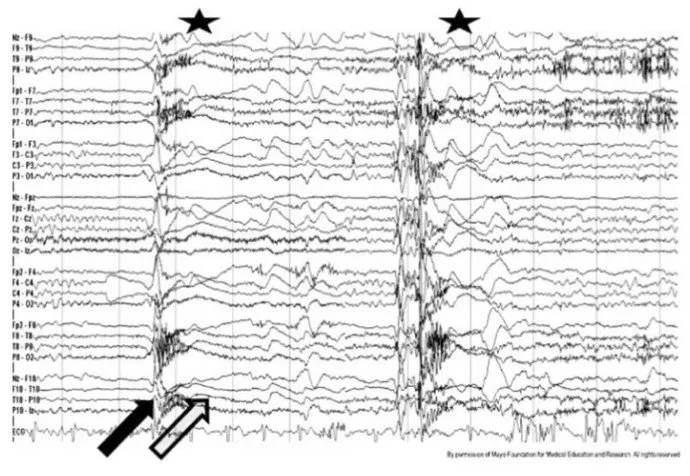
Figure 1: EEG of a Tonic Seizure.
I hope you found this blog informative. Shortly, Jaiden will be posting another blog where he will dive deeper into the neuroscience and treatments for seizures. Stay tuned!
-Jordy
References